Export a Whole Patient Chart
You can export a patient’s entire chart from PCC EHR in just a few clicks.
Video: Watch Export a Whole Patient Chart to learn more.
Stop and Think Before You Export: The patient chart export exposes all of the Protected Health Information (PHI) stored in your system for a particular patient. This information is protected by law and sharing it inappropriately may harm the patient, their caregivers, you, and your practice. Before you export a patient’s whole chart, obtain consent from the patient and share only the minimum amount of information required.
Contents
Run the Export
Export a patient’s entire chart to a password-protected file in just a few clicks.
Obtain Consent from the Patient
Ask the patient or their authorized representative for consent to share their PHI with the intended recipient of the chart export. Your practice’s global consent form might already cover this step.
Open the Patient’s Chart
Open the patient’s chart in PCC EHR.
Avoid Working in SecureConnect for Best Results: If you need to export a patient chart, avoid working in SecureConnect and use the PCC EHR desktop application instead. SecureConnect saves exports to the file system on your PCC server, which requires a follow-up call to PCC Support. By contrast, the PCC EHR desktop application saves exports to your local workstation where you can easily retrieve them and move on to your next task.
Select “Chart Export” from the Reports Menu
Once in the patient’s chart, select Chart Export from the Reports menu.
By Permission Only: Only users with the Chart Export role permission may open the Chart Export tool. For information about how to assign role permissions in PCC EHR, read Set User Roles for Permissions and Security.
Decide Whether to Include Confidential Content
The patient’s chart might include confidential notes, diagnoses, orders, and more. You can optionally include this information with the chart export.
The Chart Export window lists everything that is marked confidential in the patient’s chart. To include this information with the export, select the “Include Confidential Content” checkbox.
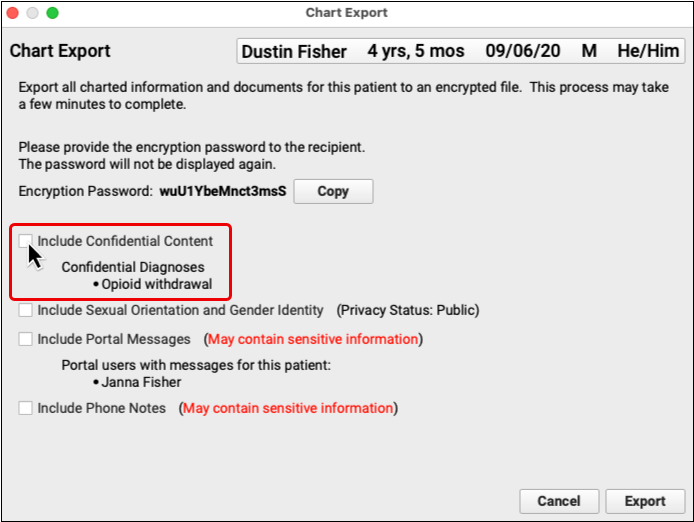
By default, confidential content is excluded from patient chart exports.
Decide Whether to Include Sexual Orientation and Gender Identity Information
Your practice might record information shared by the patient about their sexual orientation and gender identity. You can optionally include this information with the chart export.
The Chart Export window lists the privacy status of the patient’s sexual orientation and gender identity information. To include this information with the export, select the “Include Sexual Orientation and Gender Orientation” checkbox.
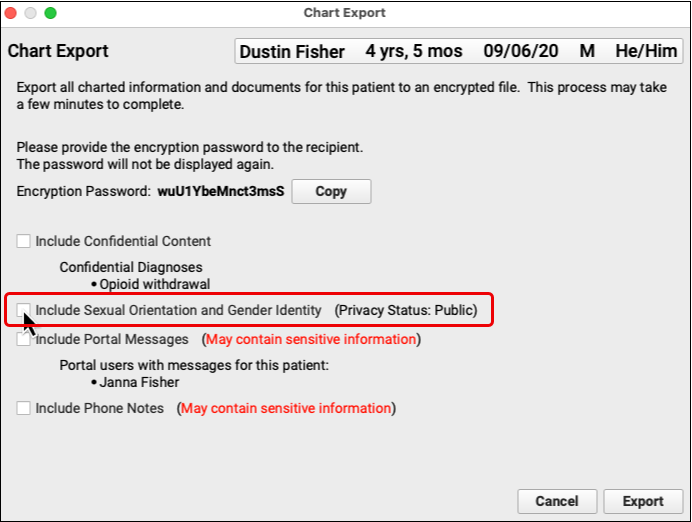
By default, sexual orientation and gender identity information is excluded from patient chart exports.
Decide Whether to Include Portal Messages
The patient might be connected to one or more portal users. You can optionally include messages from all of the patient’s portal users with the chart export.
The Chart Export window lists the patient’s portal users and each one’s relationship to the patient. To include all of these users’ messages in the chart export, select the “Include Portal Messages” checkbox.
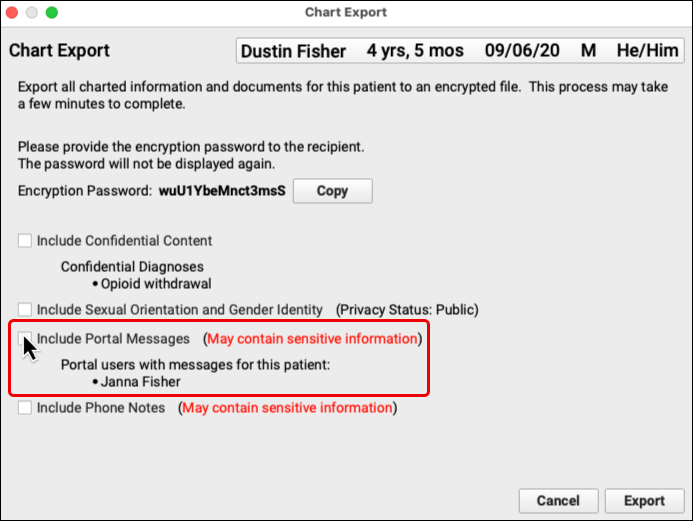
By default, portal messages are excluded from patient chart exports.
New in PCC 10.2: Decide Whether to Include Phone Notes
You can optionally include the patient’s phone notes with the chart export. To include phone notes with the chart export, select the “Include Phone Notes” checkbox.
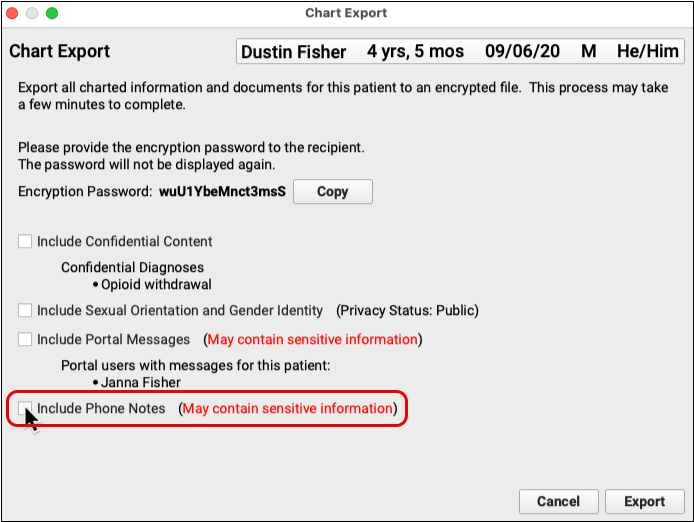
By default, phone notes are excluded from patient chart exports.
Copy the Encryption Password
Each chart export is protected by a unique encryption password. Click the “Copy” button to copy the password so that you can later share it with the recipient of the export.
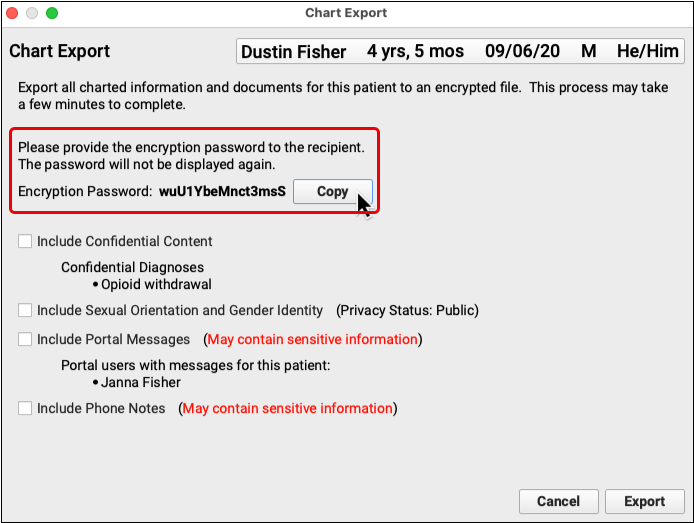
Lost Password? Generate a New Chart Export: There is no way to recover lost encryption passwords. If you or a recipient has lost the password for a past chart export, export the chart again and use a new password to access its contents.
Click “Export”
After you decide what to include with the export and copy the encryption password, click the “Export” button.
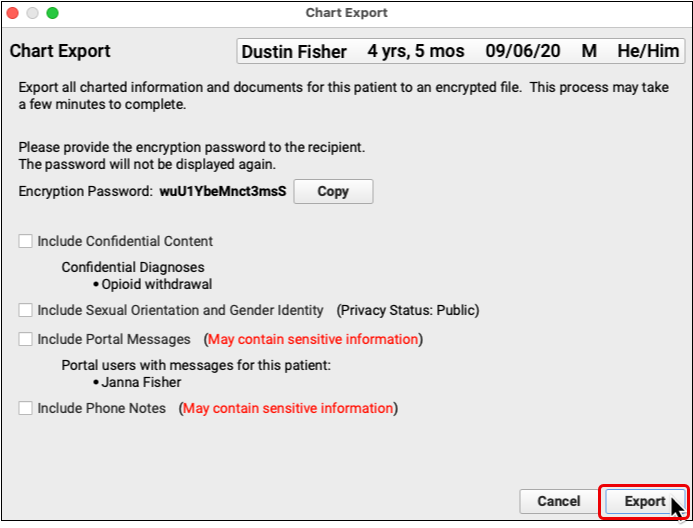
Depending on the number of visits in the patient’s history, the export may take up to a minute to complete.
Save the Export to Your Workstation
Use the file browser window to save the chart export to a location on your workstation.
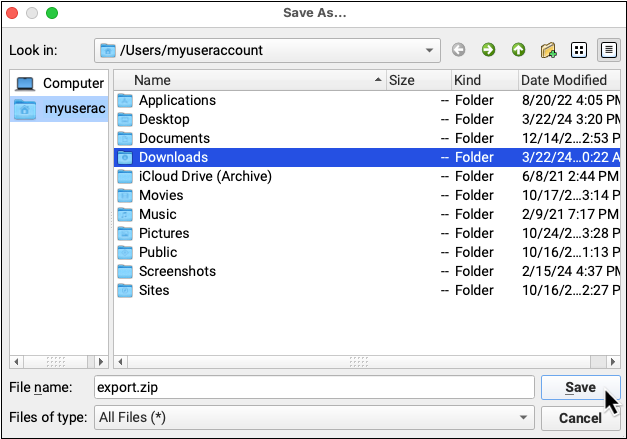
The chart export is password-protected and can safely be stored on your workstation provided the password is stored separately.
Share the Encryption Password and the Export with the Intended Recipient
Copy the encryption password into a direct secure message, portal message, or other secure type of message and send it to the recipient of the export. Then, share the export with the recipient.
You can share the export in a separate direct secure message, an email, or by putting it on a thumb drive or CD.
What’s Included
The whole patient chart export from PCC EHR includes:
- charted visits and phone notes
- demographics
- diagnoses
- all documents
- family history diagnoses
- family, medical, and social history notes
- immunizations
- lab results
- medication allergies
- medication history
- orders
- prescription history
- problems
- smoking status history
- vitals
The export automatically excludes certain information, such as confidential notes, confidential diagnoses, confidential orders, gender identity and sexual orientation information, patient portal message, and phone notes. You may opt to include this information at the time of the export.
Medications Are Always Included: For patient safety reasons, chart exports always include all medications listed in the patient’s Medication History, including those prescribed on phone note or portal message encounters.
Export Format
The patient chart export saves to a compressed, encrypted file. Use the encryption password provided with the export to decrypt and decompress the directory and access its contents.
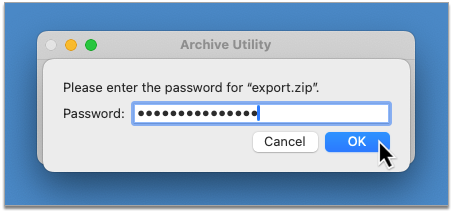
Password Prompt May Occur at Different Points: Depending on your operating system and the tool it is using to unarchive zipped folders, the prompt for the encryption password may occur when you open the encrypted directory, when you open subdirectories, or when you open the files themselves.
The top-level directory contains all of the data exported from the patient’s chart in human- and machine-readable formats (CSV, HTML, PDF, and XML).
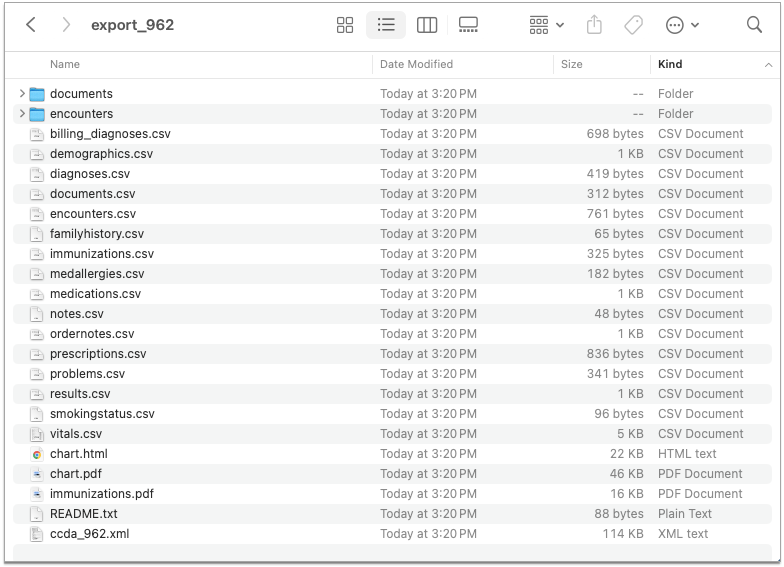
Reference the table below for descriptions of each file and subdirectory. Click any hyperlinked file name to jump to a detailed description of the data it contains.
| Name | Description | Type |
|---|---|---|
| documents | A directory containing the patient’s documents in PDF format. Documents are organized into subdirectories by type. Document types are created and assigned by the PCC practice that provides the export. Document files are named MM-DD-YYYY_ORIGINAL-FILE-NAME.pdf. | Directory |
| encounters | A directory containing the patient’s charted visits, phone notes, and portal messages (when selected for inclusion) in HTML format, as well as cascading style sheets (CSS) to style the HTML. Encounter files are named ENCOUNTER-TYPE_MM-DD-YYYY_ENCOUNTER-ID.html | Directory |
| billing_diagnoses.csv | The patient’s billed diagnoses | CSV |
| demographics.csv | The patient’s demographic information | CSV |
| diagnoses.csv | The patient’s charted diagnoses and problems | CSV |
| documents.csv | The patient’s documents | CSV |
| encounters.csv | The patient’s charted encounters, including phone notes and portal messages (when selected for inclusion) | CSV |
| familyhistory.csv | Diagnoses in the patient’s family history | CSV |
| immunizations.csv | The patient’s immunizations | CSV |
| medallergies.csv | The patient’s medication allergies | CSV |
| medications.csv | The patient’s past and present medications | CSV |
| notes.csv | The patient’s custom notes and family, social, and medical histories | CSV |
| ordernotes.csv | Free text notes associated with the patient’s orders | CSV |
| prescriptions.csv | The patient’s past and present prescriptions | CSV |
| problems.csv | The patient’s problem list diagnoses | CSV |
| results.csv | Results from the patient’s lab, screening, and other tests | CSV |
| smokingstatus.csv | The patient’s smoking status history | CSV |
| vitals.csv | The patient’s vital measurements | CSV |
| chart.html | An HTML version of the patient’s C-CDA v2.1 Continuity of Care Document (CCD) | HTML |
| chart.pdf | A PDF version of the patient’s C-CDA v2.1 Continuity of Care Document (CCD) | |
| immunizations.pdf | The patient’s school immunization form. Format varies by jurisdiction | |
| README.txt | A file containing a link to public documentation about the patient chart export and its contents. | Text |
| ccda_PATIENT-ID.xml | The patient’s C-CDA v2.1 Continuity of Care Document (CCD) | XML |
Data Structure
Learn how files in the patient chart export are structured.
billing_diagnoses.csv
This file contains a list of the patient’s billed diagnoses.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Encounter ID | The identification number of the encounter for which the diagnosis was billed |
| ICD10 Code | The International Classification of Diseases, Tenth Revision (ICD-10) code for the billed diagnosis |
| ICD10 Description | The International Classification of Diseases, Tenth Revision (ICD-10) description for the billed diagnosis |
| ICD9 Code | The International Classification of Diseases, Ninth Revision (ICD-9) code for the billed diagnosis |
| ICD9 Description | The International Classification of Diseases, Ninth Revision (ICD-9) description for the billed diagnosis |
| SNOMED Concept ID | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) code for the billed diagnosis |
| SNOMED Term | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) description for the billed diagnosis |
demographics.csv
This file contains a table of the patient’s demographic information.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Patient Last | The patient’s last name |
| Patient First | The patient’s first name |
| Patient Middle | The patient’s middle name |
| Patient Suffix | The patient’s name suffix |
| Patient Gender | The patient’s sex |
| Patient Born | The patient’s birth date |
| Custodian ID | The patient’s custodian’s PCC identification number |
| Custodian First | The patient’s custodian’s first name |
| Custodian Last | The patient’s custodian’s last name |
| Custodian Address 1 | The first line of the patient’s custodian’s home address, considered the first line of the patient’s home address |
| Custodian Address 2 | The second line of the patient’s custodian’s home address, considered the second line of the patient’s home address |
| Custodian City | The patient’s custodian’s home city, considered the patient’s home city |
| Custodian State | The patient’s custodian’s home state, considered the patient’s home state |
| Custodian Zip | The patient’s custodian’s home ZIP code, considered the patient’s home ZIP code |
| Custodian “Phone 1” | The patient’s custodian’s first phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Custodian “Phone 2” | The patient’s custodian’s second phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Custodian “Phone 3” | The patient’s custodian’s third phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Custodian “Phone 4” | The patient’s custodian’s fourth phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Primary Provider | The patient’s primary care provider (PCP) |
| Patient Race | The patient’s self-identified race |
| Patient Ethnicity | The patient’s self-identified ethnicity |
| Patient Primary Language | The patient’s primary language |
| Patient Reln to Bill Payer | The patient’s relationship to their bill payer for insurance reporting purposes |
| Guarantor ID | The patient’s guarantor’s PCC identification number |
| Guarantor First | The patient’s guarantor’s first name |
| Guarantor Last | The patient’s guarantor’s last name |
| Guarantor Address 1 | The first line of the patient’s guarantor’s home address, considered the first line of the patient’s personal billing address |
| Guarantor Address 2 | The second line of the patient’s guarantor’s home address, considered the second line of the patient’s personal billing address |
| Guarantor City | The patient’s guarantor’s home city, considered the patient’s personal billing city |
| Guarantor State | The patient’s guarantor’s home state, considered the patient’s personal billing state |
| Guarantor Zip | The patient’s guarantor’s home ZIP code, considered the patient’s personal billing ZIP code |
| Guarantor “Phone 1” | The patient’s guarantor’s first phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Guarantor “Phone 2” | The patient’s guarantor’s second phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Guarantor “Phone 3” | The patient’s guarantor’s third phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Guarantor “Phone 4” | The patient’s guarantor’s fourth phone number. The exact phone number label is decided by the PCC practice that provided the export |
| Patient Deceased Date | The patient’s date of decease |
| Sexual Orientation | The patient’s sexual orientation, if selected for inclusion in the export |
| Sexual Orientation Note | Notes about the patient’s sexual orientation, if selected for inclusion in the export |
| Gender Identity | The patient’s gender identity, if selected for inclusion in the export |
| Gender Identity Note | Notes about the patient’s gender identity, if selected for inclusion in the export |
| Preferred Pronouns | The patient’s preferred personal pronouns, if selected for inclusion in the export |
| Preferred Name | The patient’s preferred name, if selected for inclusion in the export |
diagnoses.csv
This file contains a table of the patient’s charted diagnoses.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Encounter ID | The identification number of the encounter during which the diagnosis was documented |
| ICD9 Code | The International Classification of Diseases, Ninth Revision (ICD-9) code for the diagnosis |
| ICD9 Description | The International Classification of Diseases, Ninth Revision (ICD-9) description for the diagnosis |
| SNOMED Concept ID | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) code for the diagnosis |
| SNOMED Term | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) description for the diagnosis |
| Diagnosis Note | The note associated with the diagnosis |
documents.csv
This file contains a table of the patient’s documents.
| Field | Description |
|---|---|
| Document ID | The document’s PCC identification number |
| First Page | The first page number of the document |
| Last Page | The last page number of the document |
| Encounter ID | The identification number of the encounter with which the document is associated |
| Document Date | The date the document was attached to the patient’s chart |
| Patient ID | The patient’s PCC identification number |
| Category | The category to which the document was assigned |
| Note | The note associated with the document |
| File | Where the document is stored on the exporter’s PCC system |
encounters.csv
This file contains a table of the patient’s charted visits, phone notes, and portal messages.
| Field | Description |
|---|---|
| Encounter ID | The encounter’s PCC identification number |
| Patient ID | The patient’s PCC identification number |
| Date | The date of the encounter |
| Encounter Type | The encounter type |
| Provider | The provider of the encounter |
| Note | The free-text note associated with the encounter |
| File | Where the encounter document is stored on the exporter’s PCC system |
familyhistory.csv
This file contains a table of diagnoses in the patient’s family history.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Relation | How the family member with the diagnosis is related to the patient |
| SNOMED Concept ID | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) code for the diagnosis |
| SNOMED Term | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) description for the diagnosis |
| Note | The note associated with the diagnosis |
immunizations.csv
This file contains a table of the patient’s immunizations.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Description | The name of the immunization |
| CVX | The Vaccine Administered (CVX) code for the vaccine |
| Site | The site where the vaccine was administered |
| Manufacturer | The company that manufactured the vaccine |
| Lot | The vaccine lot number |
| VIS | The identification number of the Vaccine Information Sheet (VIS) provided to the patient when the vaccine was administered |
| VIS Date | The Vaccine Information Statement (VIS) publication date |
| Encounter ID | The identification number of the encounter during which the vaccine was administered |
| Date | The date the vaccine was administered |
| Status | The status of the vaccine administration |
| Notes | Free text notes associated with the vaccine |
medallergies.csv
This file contains a table of the patient’s medication allergies.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Allergen | The text description of the allergen |
| Allergen Code | The First Data Bank (FDB) code for the allergen |
| Allergen Code System | The code system employed for allergy documentation |
| Sensitivity Type | The patient’s sensitivity type to the allergen |
| Sensitivity Type Code | The First Data Bank (FDB) code for the sensitivity type |
| Severity | The severity of the patient’s allergy |
| Severity Code | The First Data Bank (FDB) code for the severity of the patient’s allergy |
| Reaction | The patient’s reaction to the allergen |
| Onset Date | The onset date for the allergy |
| Resolved Date | The date the allergy resolved |
| Active | The active status of the allergen |
medications.csv
This file contains a table of the patient’s past and present medications.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| ndc_id | The National Drug Code (NDC) for the medication |
| rxnorm_codes | The RxNorm code for the medication |
| drug_description | A description of the medication |
| pat_language_drug_description | A patient-friendly description of the medication |
| drug_name | The name of the medication |
| directions | Directions for taking the medication |
| pat_language_directions | Patient-friendly directions for taking the medication |
| route_code | The route for taking the medication |
| dose | The quantity of medication per dose |
| dose_units | The dose unit of measure |
| drug_strengths | The medication strength |
| pat_language_drug_strengths | A patient-friendly description of the medication strength |
| frequency_code | The frequency with which the patient was instructed to take the medication |
| instructions | Free-text instructions describing how to take the medication |
| comments | Non-patient-facing comments about the medication |
| duration | The duration of the medication |
| duration_units | The time units for the duration of the medication |
| start_date | The date the patient was instructed to start taking the medication |
| stop_date | The date the patient was instructed to stop taking the medication |
| discontinued_ts | The date the medication was discontinued in the patient’s medication history |
| prescriber_name | The name of the person who prescribed the medication |
| active | The active status of the medication |
notes.csv
This file contains a table of the patient’s custom notes and family, social, and medical histories.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Note Type | The type of the note |
| Note | The contents of the note |
| Last Modified | The date the note was last modified |
ordernotes.csv
This file contains a table of free text notes associated with the patient’s orders.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Encounter ID | The identification number of the encounter during which the order was placed |
| Order ID | The order’s PCC identification number |
| Order Code | The order’s PCC order code |
| Order Name | The name of the order |
| Order Date | The date the order was placed |
| Note Date | The date that the note was saved |
| Discrete Result | A flag indicating whether the result values are discrete or non-discrete (1 is discrete, 0 is non-discrete) |
| Note | The free-text note associated with the order |
prescriptions.csv
This file contains a table of the patient’s past and present prescriptions.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Encounter ID | The identification number of the encounter during which the prescription was created |
| ndc_id | The National Drug Code (NDC) for the prescribed medication |
| rxnorm_codes | The RxNorm code for the prescribed medication |
| drug_description | A description of the prescribed medication |
| pat_language_drug_description | A patient-friendly description of the prescribed medication |
| drug_name | The name of the prescribed medication |
| directions | Directions for taking the prescribed medication |
| pat_language_directions | Patient-friendly directions for taking the prescribed medication |
| drug_strengths | The strength of the prescribed medication |
| pat_language_drug_strengths | A patient-friendly description of the prescribed medication strength |
| comments | Non-patient-facing comments about the prescribed medication |
| start_date | The date the patient was instructed to start taking the prescribed medication |
| stop_date | The date the patient was instructed to stop taking the prescribed medication |
| discontinued-ts | The date the prescribed medication was discontinued in the patient’s medication history |
| prescriber_name | The name of the person who prescribed the medication |
| quantity | The total quantity that was prescribed |
problems.csv
This file contains a table of the patient’s problem list diagnoses, including non-medication allergies.
ICD9 DescriptionThe Internal Classification of Diseases (ICD-10) description for the problem list diagnosis
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| ICD9 Code | The Internal Classification of Diseases (ICD-10) code for the problem list diagnosis |
| SNOMED Concept ID | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) code for the problem list diagnosis |
| SNOMED Term | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) description for the problem list diagnosis |
| Resolved Date | The date the problem resolved |
| Onset Date | The onset date of the problem |
| Status | The active status of the problem |
| Inactive Date | The date the problem list diagnosis was marked inactive |
| Problem Note | The free-text note associated with the problem list diagnosis |
| Allergy | A binary flag indicating whether the problem is an allergy (0 for no, 1 for yes) |
results.csv
This file contains a table of results from the patient’s lab, screening, and other tests.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Encounter ID | The identification number of the encounter during which the test associated with the result was ordered |
| Order ID | The identification number of the PCC order associated with the result |
| Result Set ID | The identification number of the set to which the result belongs |
| Seq# | Where the result appears in sequence within the result set |
| LOINC Code | The Logical Observation Identifiers Names and Codes (LOINC) code for the test associated with the result |
| Value | The discrete result value |
| Result Text | A description of the test associated with the result |
| Units | If applicable, the unit of measure for the discrete result value |
| Interpretation Code | The interpretation code for the result as defined by the HL7 v2.5.1 Abnormal Flags table |
| Normal Range | The range in which the result must fall to be considered normal |
| Abnormal | A binary flag indicating whether the result is abnormal (0 for no, 1 for yes) |
| Result Date | The date and time the result was reported |
| Note | The free-text note associated with the result |
| Order Name | The name of the PCC order associated with the result |
| Order Type | The type of the PCC order associated with the result |
smokingstatus.csv
This file contains a table of the patient’s smoking status history.
| Field | Description |
|---|---|
| Patient ID | The patient’s PCC identification number |
| Encounter ID | The identification number of the encounter during which the smoking status was documented |
| SNOMED Code | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) code for the smoking status |
| SNOMED Term | The Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) description for the smoking status |
vitals.csv
This file contains a table of the patient’s vital measurements.
| Field | Description |
|---|---|
| Encounter ID | The identification number of the encounter during which the vital measurement was taken |
| Patient ID | The patient’s PCC identification number |
| Vital Type | The vital type |
| Major Value | The major value of the vitals measurement |
| Major Unit | The unit of measure for the major value |
| Minor Value | The minor value of the vitals measurement |
| Minor Unit | The unit of measure for the minor value |
| Temperature Method | How the patient’s temperature was measured |
| Blood Pressure Location | Where the patient’s blood pressure was measured |
| Blood Pressure Position | The position the patient was in when their blood pressure was measured |
| Date | The date of the vitals measurement |
| Percentile | How the patient’s vitals measurement compares to others in a range |
| Percentile Source | The source of the range used for calculating the percentile |
chart.html, chart.pdf
A human-readable version of the patient’s C-CDA v2.1 Continuity of Care Document (CCD).
| Section | Description |
|---|---|
| Patient, Document, and Sender Details | Patient, document, and sender identifying information. Includes patient name, date of birth, sex, race, ethnicity, contact information, and IDs; document ID and creation date; primary care provider name, authoring system, and workplace address; maintaining organization name and workplace address. |
| Table of Contents | A hyperlinked list of sections included in the Continuity of Care Document (CCD). |
| Allergies, Adverse Reactions, Alerts | A list of the patient’s allergies. Includes allergen code, name, reaction note, onset date, and active status. |
| History of Medication Use | A list of the patient’s past and present medications. Includes medication code, brand name, strength, route, form, start date, and stop date. |
| Problem List | A list of the patient’s problem list diagnoses. Includes diagnosis name, SNOMED-CT/ICD-9 code, onset date, and active status. |
| History of Procedures | A list of the patient’s past and present procedures. Includes order name, SNOMED code, SNOMED description, procedure date, and completion status. |
| Relevant Diagnostic Tests and/or Laboratory Data | A list of the patient’s lab, screening, and other diagnostic tests. Includes result types, SNOMED codes, descriptions, dates, statuses, and results. |
| Vital Signs | A list of the patient’s vital sign measurements. Includes vital type, value, unit, and date taken. |
| Social History | A list of the patient’s social history notes. Includes date recorded, SNOMED code, and status. |
| Care Plan | The patient’s care plan(s). |
| Immunizations | A list of the patient’s immunizations. Includes vaccine, date administered, site, and status. |
| Encounters | A list of the patient’s charted encounters. Includes encounter type, performer, location, date, and diagnoses. |
| Reason for Referral | A list of referral reasons. Includes result type, SNOMED code, description, date, status, and result. |
| Functional Status Assessment | Notes about the patient’s cognitive or functional status. |
| Payers | The patient’s insurance policies. Includes policy order indicator, policy name, certificate number, group number, and phone number. |
Additional Information
There are a few more things you should know about patient chart exports in PCC EHR.
Who to Contact
If you received a patient chart export and have questions about its contents, contact the practice who provided the export.
If you are a PCC practice with questions about the export, contact PCC Support.
Multi-Patient Chart Exports
If you need access to information beyond what is provided with the patient chart export tool and PCC reports, such as detailed audit logs or a multi-patient chart export, contact PCC Support.
Depending upon the complexity of the request and the degree of developer involvement required, special data exports may carry an additional fee.