Code and Bill for E&M Office Visits
Upon completion of a sick visit encounter, a clinician selects an “Evaluation and Management” or E&M code. This is sometimes called the “office visit” level. E&M level selection is based on the clinician’s medical decision making or the amount of time spent on care for that patient on the calendar date of the encounter.
Procedure Code Guidance: The procedure codes discussed in this article are intended only as examples. You should consult the AMA’s current CPT Coding Guide and work with your insurance payers to verify what codes you should report on claims. Your practice updates and maintains your billable procedure list, codes, and prices in the Procedures table in the Tables configuration tool on your PCC system.
Contents
Why is E&M Code Selection Important to a Pediatric Practice?
E&M services make up a large percentage of the work you do as a pediatrician. They represent the cognitive work, information gathering, and decision making that goes into patient care. Because so much of the work you do falls under the umbrella of E&M, it’s vital that you code those services correctly. Many pediatricians under-code their encounters, resulting in significant lost revenue for their practice.
Documenting your encounters is not only important for continuity of care. It also supports collecting and retaining the revenue those services generate.
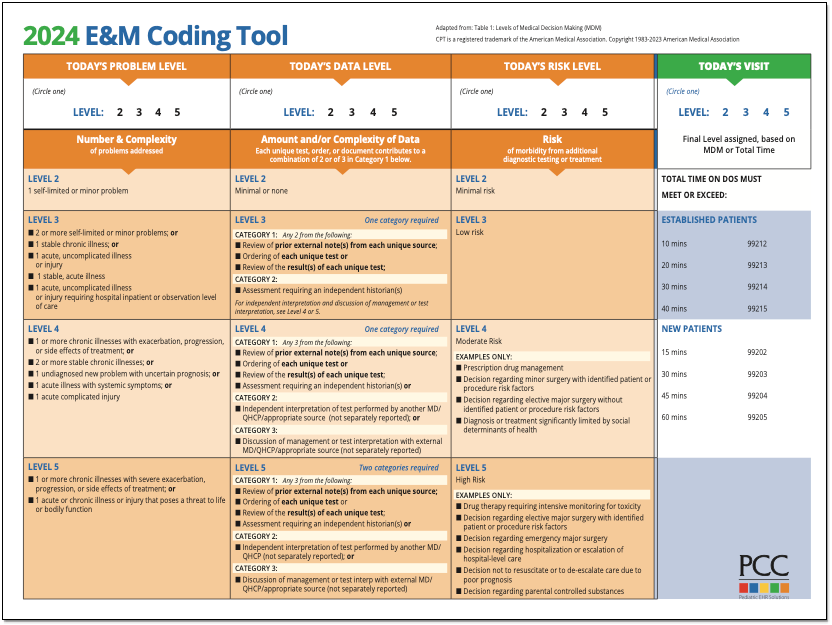
PCC’s E&M Coding Tool
PCC’s Jan Blanchard (CPC, CPEDC) developed a printable guide for E&M Coding.
2021 Transition Resources Archive
On January 1st, 2021, the guidelines for coding and billing an office visit changed significantly. PCC collected resources, created tutorials, and managed an FAQ at that time.
2021 Resource Guide: Some of the details below have changed since 2021. You should consult the current AMA CPT Coding Guide for the most up to date requirements and guidance. Reach out to PCC Support or attend a live PCC Billing Drop-In session to learn more.
How Do I Select an E&M Code for 2021 and Beyond?
For encounters that occur after December 31st, 2020, a clinician no longer uses history or physical exam performed during the encounter as criteria for code selection. Instead, they select a code based on either medical decision making or time spent practicing care for the patient on the day of the visit.
Here’s a brief explanation of how you select a billing code level for an “evaluation and management” or “Office Visit” after January 1st, 2021. These guidelines apply to common visit billing codes, such as 99212, 99213, 99214, or 99215, as well as to the selection of codes 99202 through 99205.
Select a Code Based on Medical Decision Making
You can base your visit level code on medical decision making, which is comprised of three elements:
-
Problems Addressed: The number of problems you addressed for the patient during the day of the encounter.
-
Items Reviewed: The tests, chart information, and other data you reviewed in relation to the problems addressed today.
-
Risk: The level of risk presented to the patient.
- 2021 Evaluation and Management Updates: What changed? This 15 minute video explains the new way of selecting E&M codes in context with how you coded sick office visits before.
- PCC’s 2021 E&M FAQ&A: Frequently asked questions, and a live Q&A about 2021 E&M leveling.
- 2021 E&M Workshop: A live workshop led by PCC, this session includes an overview of the changes and examples of real-world level selection.
- The Impact of 2021 E&M Coding Changes on Pediatrics: Learn about the E&M coding changes in context, and then hear PCC’s ideas about how these changes will affect the business of pediatrics.
- Pediatric Management Institute’s September COVID-19 Webinar: During the September 2020 session of the PMI’s ongoing webinar series, The Business Impact Of COVID19 On Pediatric Practices, this topic is covered along with other current topics. This recorded live webinar includes some additional Q&A.
- PCC Resources
-
Evaluate Your Practice's E&M Habits and Patterns: Your Practice Vitals Dashboard, available from within PCC EHR, provides a number of metrics, tools and recommendations related to E&M coding included on the “E&M Coding Distribution” measure.
-
Confessions of a Pediatric Practice Management Consultant: PCC’s Chip Hart runs a blog and podcast, covering many topics related to practice management, including E&M coding. You can find it here.
-
- Other Resources
- AAP FAQ: E&M 2021 coding questions and answers by the American Academy of Pediatrics.
- AAP MDM Grid: A direct link to the AAP’s chart which illustrates levels of medical decision making. It includes several useful examples. (AAP hosts this file here.)
- MDM Tracker: An online tool for selecting visit level based on medical decision making in 2021.
-
Where can I find PCC’s 2021 MDM Tool?Here it is: PCC’s 2021 E&M Coding Tool.
-
Where can I find the online MDM calculator Chip Hart shared?You can find it on the Confessions of a Pediatric Practice Management Consultant blog post entitled “Free E&M Medical Decision Making Calculator”.
-
Is fever a systemic symptom which can elevate a visit’s level?Sometimes. It depends on the patient’s presentation, and only when paired with an acute illness.
CPT defines systemic symptoms this way:
“Acute illness with systemic symptoms: An illness that causes systemic symptoms and has a high risk of morbidity without treatment. For systemic general symptoms, such as fever, body aches, or fatigue in a minor illness that may be treated to alleviate symptoms, shorten the course of illness, or to prevent complications, see the definitions for self-limited or minor problem or acute, uncomplicated illness or injury. Systemic symptoms may not be general but may be single system. Examples may include pyelonephritis, pneumonitis, or colitis.” (p12-14 2021 CPT Manual)Fever had become a mainstay of complexity expression in E&M documentation. In 2021, not all fevers meet the definition of a systemic symptom. AMA says that in cases where the fever is a “general symptom in a minor illness”, it is *not* systemic. So using it to express visit complexity becomes a case-by-case determination for 2021. Things like age and other risks will be determining factors that clinicians will have to consider when they decide this point.
-
Can we get points for both ordering and reviewing tests and labs in our MDM leveling?No. For any one test or lab, you may include *either* the ordering or reviewing done on the service date. To include both points would be “double dipping”.
Furthermore, the AAP has interpreted the AMA’s position to be that you may not consider tests performed in your office in your MDM level determination. This interpretation is under review.
-
Will documenting multiple diagnoses lead to a higher level of MDM?
Maybe. “Problems” are the units of determination for MDM. So, if you treat three problems in a visit, but there are five ICDs listed, the ICDs do not inherently support higher complexity leveling. Some ICDs are reported because they represent circumstances and/or problems which complicate care but which are not specifically addressed at that visit. Documenting the role that those existing problems play in your thinking could support assigning higher Problem values to what *is* addressed.
-
Can I really get credit every time a parent or guardian contributes history to a visit?Maybe. If you feel confident that the contribution they made is required for appropriate care to be rendered, yes. Document the reason for their perspective being necessary if it is not obvious. For example, little ones who can’t speak for themselves obviously require someone to give their history. But for teens, the necessity of another perspective in, say, behavioral or social concerns where objective input is valuable, document a statement to that effect and take the independent historian point(s).
-
If I spend time reviewing records from a different practice, even if they’re from a practice where I formerly practiced medicine, can I count that time toward my day’s total?Technically, I would say yes. If the patient is familiar to you, the review would likely not take very long, necessarily.
Follow Up Question: What if I am reviewing records at my practice that are “old”, say, greater than 3 yrs?
Answer: No, not the way requirements are currently written: “Review of prior external note(s) from each unique source.” Only records from sources outside your own organization can be considered external and valid for those points. -
How do Social Determinants of Health (SDoH) count toward MDM?Per CPT 2021, SDoHs are “Economic and social conditions that influence the health of people and communities. Examples may include food or housing insecurity.”
Per the Elements of Medical Decision Making grid published by AMA in CPT® Evaluation and Management (E/M) Office or Other Outpatient (99202-99215) and Prolonged Services (99354, 99355, 99356, 99XXX) Code and Guideline Changes, an example of Moderate risk of morbidity from additional diagnostic testing or treatment is “Diagnosis or treatment significantly limited by social determinants of health”. I interpret these references to suggest that any SDoH which significantly limits the patient’s ability to carry out the clinician’s plan meets the Level 4 risk requirement.
According to the U.S. Department of Health, Social Determinants of Health are economic and social conditions that influence the health of people and communities. Their examples include:
- Safe housing, transportation, and neighborhoods
- Racism, discrimination, and violence
- Education, job opportunities, and income
- Access to nutritious foods and physical activity opportunities
- Polluted air and water
- Language and literacy skills
Some of these may be reported using ICD codes found in “Persons with potential health hazards related to socioeconomic and psychosocial circumstances Z55-Z65”
- Z55 Problems related to education and literacy
- Z56 Problems related to employment and unemployment
- Z57 Occupational exposure to risk factors
- Z59 Problems related to housing and economic circumstances
- Z60 Problems related to social environment
- Z62 Problems related to upbringing
- Z63 Other problems related to primary support group, including family circumstances
- Z64 Problems related to certain psychosocial circumstances
- Z65 Problems related to other psychosocial circumstances
-
How will billing sick care that was rendered during a well visit be affected by the 2021 E&M changes?As a physical exam is not a consideration in leveling 2021 E&M visits, clinicians can now capture sick care for New Patient well visits, and can more easily level any visit that includes both sick and well care.
The new MDM focus on visit leveling represents less subjectivity in discerning which parts of a service were part of the well care and which were part of the sick care.
-
Do I need to document in the note the exact amount of time spent on each activity, or is it ok to just document total time?Full day totals are permissible, but I would feel better seeing at least time segments. Rough estimates for segments would do, but to expect that human brains can recreate a day’s worth of timed detail accurately for work that gets interrupted and broken up and then wrapped up after everyone else has gone home is a stretch which can be avoided.
-
Is there still a Level 1 visit for nurse-only visits?Yes, for established patients only, a Level 1 nurse visit can be reported using 99211. New patient level 1 code 99201 expires on 12/31/20 and is not reportable thereafter. This is due to the identical MDM requirements for both 99201 and 99202. By 2021 standards, 99201 becomes redundant to 99202.
-
If I continue to chart after hours, can I add that time for the purposes of leveling the visit?Yes. Caveat: The only after hours charting time (or any other clinical activity time) you may include in your billed time is the time spent *on the date of service*. If you chart any part of yesterday’s visit today, you may bill by time but you cannot include the time you spent today in the total you use for choosing your level. For example, if on Monday you see an established patient and spend 5 minutes reviewing records, 10 minutes in a visit, 5 minutes on a results call Monday night and 10 minutes charting on Tuesday morning, you may only bill a level 3 visit using Monday time: 5+10+5=20 minutes; Tuesday’s 10 minutes cannot count toward the leveling.
-
Will I get MDM data points for tests like rapid flu or rapid strep for which I also charge?Currently, no. The current interpretation of the relationship between awarding data points for tests and labs and paying for tests and labs is that they are mutually exclusive.
Discussions around this continue, but currently you should not expect to level using data points for test and labs you bill.
-
Are a CBC and differential counted as more than 1 lab? Or for example COVID-19/Flu/RSV combo - is that 1 test or 4 tests?It depends on the number of CPTs. If CBC and differential are one CPT, it is one data point for either ordering or reviewing. If the COVID-19/Flu/RSV combo is one CPT, one point is its data value.
-
Could I count one of several screenings towards data reviewed and bill for the other and not be double-dipping?This is not in the spirit of the requirement, but is still under discussion. Billing effects are impossible to explore here. The sheer variety of payers and policies means the outcome can not be predicted. Furthermore, carrier behavior makes predictions of future claim determinations little more than a guessing game.
-
Do I get credit if some historians are in office and others participate over facetime, phone, etc., for the same visit?Yes. There is no cumulative credit for historians, but if someone other than the patient is required to participate that requirement is met.
-
If you use a formal screen for SDoH that is scored and payable, then you can’t count that screening towards MDM, correct?Currently, that is correct.
-
Does pulse oximetry give a data point?I don’t know, and this question is more complex than it looks. The debate between clinicians about whether pulse ox is a vital sign is a factor. If you consider it a vital, it is not a test, and counting it as a data point is questionable. However, pulse ox has a billable CPT, so some may consider it a test.
Also, the question of whether in-house tests and labs may be used for data credit remains unanswered. I am undecided on this as yet and will count on the clinicians with whom I review encounters to help me arrive at a position on this point in future.
-
We do our huddle and "run the schedule" (i.e. review referrals, lab results, vaccines, and consult notes) the day *before*, not the day of! Can we count that time when leveling each of those encounters?No. Currently, the only “billable” time is that spent by the clinician for that patient on the service date.
-
Does 'undiagnosed new problem with uncertain prognosis' relate to when we don’t yet have a diagnosis, or does it mean a new previously undiagnosed problem that you identified at the visit?This phrase comes from a MDM requirement. Our interpretation is that it means a new problem for the patient that you have never seen before, and for which you are uncertain of the outcome.
CPT 2021 is light on guidance on this point. “Undiagnosed new problem with uncertain prognosis: A problem in the differential diagnosis that represents a condition likely to result in a high risk of morbidity without treatment. An example may be a lump in the breast…” The AAP offered an additional example of a potentially malignant lesion in the Feb 2020 issue of the Coding Newsletter.
-
If we bill for one Vanderbilt, could we then claim MDM credit for the ones from other sources?My sense of this is that doing so is *not* in the spirit of the guideline. Additionally, performing a service and not billing for it will run afoul of many insurance contracts. Also, please see above for information about Data credit for in-house labs and tests.
-
What about the hand-on-the-doorknob minor things that parents like to bring up? If there are enough of these, or significant ones, can I document them in a manner that might bump MDM up a level?
Example: Rash (insect bite) + been a little constipated (give some prune juice), been having stomach aches (few questions to make sure it’s nothing worrisome, asked to schedule another visit to evaluate further)…
Yes, but MDM is based on significance, not the number of problems. The total number of problems does not necessarily increase the credit you can claim for complexity in the Number and Complexity of Problems Addressed element. Rather, the most complex problem addressed (Minimal, Low, Moderate, High) in a given encounter typically represents the level of “problems addressed” which should be used for leveling. Exceptions include self-limited, minor problems (1 = Minimal while 2 = Low) and stable chronic illnesses (1 = Low, 2 = Moderate).
-
Can concussion be considered an acute complicated injury - a head injury that gave other systemic symptoms?Described that way, absolutely. Be sure to familiarize yourself with the AMA’s definition of Systemic Symptoms.
-
What is meant by 'risk'? The guideline only lists examples. Is there a way to determine risk on MDM without these examples? Is that purely a judgment call?Yes, this is a clinical judgment.
From the AMA: “Trained clinicians apply common language usage meanings to terms such as high, medium, low, or minimal risk and do not require quantification for these definitions (though quantification may be provided when evidence-based medicine has established probabilities). For the purposes of MDM, level of risk is based upon consequences of the problem(s) addressed at the encounter when appropriately treated. Risk also includes MDM related to the need to initiate or forego further testing, treatment, and/or hospitalization.”
-
If you send a kid to the Emergency Department, or for testing due to concern for appendectomy, does that discussion get you to a higher level of risk? Does discussion of a possible ER visit count?Not usually. If the decision is purely for testing consideration, meaning the tests could be done in another care setting without ready access to acute or surgical or inpatient care, I would *not* say that meets the spirit of the requirement.
From the AMA: “… decision about hospitalization includes consideration of alternative levels of care…Examples may include a psychiatric patient with a sufficient degree of support in the outpatient setting or the decision to not hospitalize a patient with advanced dementia with an acute condition that would generally warrant inpatient care, but for whom the goal is palliative treatment.”
-
Will PCC develop a software timer to capture clinician charting time?PCC is not currently developing a timer in PCC EHR. Our research mid-2020 about this feature found that users did not see enough value in having to activate a timer whenever they turned their attention to a particular chart.
For example, if PCC EHR automatically records your time with a chart open, you would be required to close and reopen every chart every time you were interrupted while charting in order for it to be accurate. If you had to actively click a button to stop and start a timer, it would be an ever-present timer that required their attention. Users shared this would be distracting at best and annoying at worst. Most users were happier to state their own estimates of how much time was spent, either in total or in segments to be used for totaling when they were sure services were complete for the whole day.
Select a Code Based on Time
You can base your visit level code selection on the total time that the rendering clinician spent on the patient that day. That can include the time the pediatrician spent before, during, and after the actual encounter.
Watch PCC 2021 E&M Coding Videos
These 2021 videos provide examples of how to level your E&M visits:
Configure PCC EHR to Support Your Clinicians and Billers for E&M Level Selection in 2021
Your practice can add fields to your chart note protocols in order to track time spent before, during, and after the encounter by the clinician. You can also track the number of problems addressed, items reviewed for the problems, and the level of risk present.
As an example, this sample chart note protocol includes components designed to quickly note problems, time and risk.
For help customizing your protocols, check out Configure Chart Note Protocols, and get in touch with PCC Support for assistance.
2021 Additional Resources and Guides
In the lead up to the 2021 transition, PCC published blog posts and other organizations published guides and online tools.
2021 Questions and Answers on Interpreting E&M Guidelines
PCC’s Jan Blanchard works with pediatric practices to help them interpret coding guidelines. Read below to see a selection of the 2021 E&M questions received at the time of the transition. These Q&As were last updated on 2021-01-08, so you should consult your AMA CPT Guide for more recent details.